Introduction of Conn’s Syndrome and Pheochromocytoma
Conn’s Syndrome: Conn’s Syndrome, or primary hyperaldosteronism, is a rare adrenal gland disorder characterized by excess aldosterone production. Aldosterone regulates sodium and potassium balance, and when overproduced, it can lead to high blood pressure and electrolyte imbalances, posing significant health risks.
Pheochromocytoma: Pheochromocytoma is a rare tumor of the adrenal medulla that triggers excessive catecholamine release, causing severe blood pressure spikes, palpitations, sweating, and other intense symptoms. Understanding these adrenal disorders is essential for timely diagnosis and treatment.
A brief overview of adrenal gland disorders
Adrenal gland disorders are a group of medical conditions that affect the adrenal glands, which are small, triangular-shaped organs located on top of each kidney. These glands play a crucial role in producing hormones that regulate various bodily functions.
Here’s a brief overview of adrenal gland disorders:
- Adrenal Insufficiency:
- Also known as Addison’s disease, adrenal insufficiency occurs when the adrenal glands don’t produce enough hormones, particularly cortisol and sometimes aldosterone.
- Symptoms include fatigue, weight loss, muscle weakness, low blood pressure, and skin changes.
- It can be caused by autoimmune conditions, infections, or other underlying diseases.
- Cushing’s Syndrome:
- Cushing’s syndrome results from an excess production of cortisol, often caused by tumors in the adrenal glands (adrenal adenomas) or excessive use of corticosteroid medications.
- Symptoms include weight gain, high blood pressure, muscle weakness, and changes in the appearance of the skin (e.g., thinning and easy bruising).
- Conn’s Syndrome (Primary Hyperaldosteronism):
- Conn’s syndrome occurs when the adrenal glands produce too much aldosterone, a hormone that regulates sodium and potassium balance.
- Common symptoms include hypertension (high blood pressure), muscle weakness, and low potassium levels (hypokalemia).
- It is often caused by adrenal gland tumors or hyperplasia.
- Pheochromocytoma:
- Pheochromocytoma is a rare tumor of the adrenal glands that produce excessive amounts of catecholamines (e.g., adrenaline).
- Symptoms include paroxysmal (sudden and severe) hypertension, palpitations, sweating, and anxiety attacks.
- Adrenal Tumors:
- Adrenal tumors can be benign (non-cancerous) or malignant (cancerous).
- They can cause a variety of symptoms depending on their type and size, including abdominal pain, weight loss, and hormonal imbalances.
- Congenital Adrenal Hyperplasia (CAH):
- CAH is a genetic disorder in which the adrenal glands produce abnormal amounts of steroid hormones, leading to hormonal imbalances.
- Symptoms vary depending on the specific hormone affected and may include ambiguous genitalia in females and salt-wasting in both sexes.
- Adrenocortical Carcinoma:
- This is a rare cancer that originates in the adrenal cortex (the outer part of the adrenal gland).
- It can cause a variety of symptoms, including abdominal pain, weight loss, and hormonal disturbances.
Treatment for adrenal gland disorders depends on the specific condition and its underlying cause. It may involve medication, surgery to remove tumors, hormone replacement therapy, or a combination of these approaches. Early diagnosis and management are crucial for effectively managing adrenal gland disorders and preventing complications.
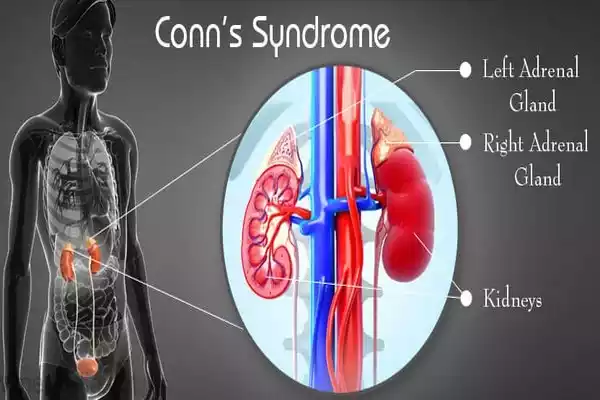
Anatomy and Function of Adrenal Glands
The adrenal glands are a pair of small, triangular-shaped organs located on top of each kidney. Despite their relatively small size, these glands play essential roles in the endocrine system and overall physiological regulation.
Here’s an overview of the anatomy and function of the adrenal glands:
Anatomy of the Adrenal Glands:
- Adrenal Cortex: This is the outer layer of the adrenal gland and accounts for about 80-90% of the gland’s mass. It is subdivided into three zones, each responsible for producing specific hormones:
- Zona Glomerulosa: This outermost layer produces mineralocorticoids, primarily aldosterone, which regulates electrolyte and water balance in the body.
- Zona fasciculata: The middle layer produces glucocorticoids, primarily cortisol. Cortisol plays a key role in regulating metabolism, immune response, and the body’s stress response.
- Zona Reticularis: The innermost layer produces androgens, which are weak male sex hormones. These hormones have various functions, including the development of secondary sexual characteristics.
- Adrenal Medulla: This is the inner core of the adrenal gland, and it is responsible for producing catecholamines, such as adrenaline (epinephrine) and norepinephrine. These hormones are crucial for the body’s fight-or-flight response and help prepare the body to respond to stress.
The function of the Adrenal Glands:
- Hormone Production: The adrenal glands produce a range of hormones that regulate various physiological processes:
- Cortisol: Produced by the zona fasciculate, cortisol influences metabolism, regulates blood sugar levels, and helps the body respond to stress. It also has anti-inflammatory properties.
- Aldosterone: Produced by the zona glomerulosa, aldosterone controls the balance of sodium and potassium in the body. It helps maintain blood pressure and electrolyte balance.
- Androgens: The zona reticularis produces small amounts of androgens, which contribute to the development of secondary sexual characteristics, particularly in women.
- Stress Response: The adrenal medulla produces adrenaline and norepinephrine, which are released into the bloodstream in response to stress or perceived threats. These hormones increase heart rate, raise blood pressure, and prepare the body for “fight or flight” by redirecting blood flow to vital organs and muscles.
- Fluid and Electrolyte Balance: Aldosterone helps regulate the balance of sodium and potassium in the body. It acts on the kidneys to increase the reabsorption of sodium and the excretion of potassium, which helps maintain blood pressure and electrolyte equilibrium.
- Secondary Sexual Characteristics: The adrenal androgens, though produced in small quantities compared to the gonads (testes and ovaries), contribute to the development of secondary sexual characteristics like body hair growth and libido.
The adrenal glands are essential endocrine organs that produce hormones critical for regulating metabolism, responding to stress, maintaining fluid and electrolyte balance, and influencing secondary sexual characteristics. Dysfunction of the adrenal glands can lead to a range of medical conditions and hormonal imbalances.
Conn’s Syndrome
Conn’s Syndrome, also known as primary hyperaldosteronism, is a rare medical condition characterized by the overproduction of the hormone aldosterone by the adrenal glands.
Aldosterone is a hormone produced by the adrenal cortex, specifically in the zona glomerulosa, and it plays a crucial role in regulating the balance of sodium and potassium in the body. When there is excessive production of aldosterone, it can lead to electrolyte imbalances and high blood pressure (hypertension).
Causes and Mechanism: The most common cause of Conn’s Syndrome is the presence of a benign tumor called an aldosterone-producing adenoma, which forms within one of the adrenal glands. These tumors result in the increased production of aldosterone independent of the body’s normal regulatory mechanisms. In some cases, Conn’s Syndrome can also be caused by bilateral adrenal hyperplasia, which involves the overgrowth of adrenal tissue.
Symptoms: The primary effects of Conn’s Syndrome stem from the hormonal imbalances it causes, specifically an excess of aldosterone. Common symptoms and manifestations include:
- Hypertension: High blood pressure is a hallmark of Conn’s Syndrome. It is often difficult to control with standard antihypertensive medications and may require specific treatment approaches.
- Hypokalemia: Due to excessive aldosterone, the body retains sodium and excretes potassium in the urine. This leads to low levels of potassium in the blood, which can cause muscle weakness, fatigue, and even cardiac arrhythmias.
- Muscle Weakness: Low potassium levels can affect the function of muscles, leading to weakness and sometimes even paralysis.
- Polyuria and Polydipsia: Increased urination and thirst are often observed due to the effects of aldosterone on fluid balance and electrolyte regulation.
Diagnosis: Diagnosing Conn’s Syndrome involves a combination of clinical assessment and specific tests:
- Blood Tests: Measuring aldosterone and renin levels in the blood can help identify an abnormal aldosterone-to-renin ratio.
- Imaging: Techniques like CT scans or MRI can locate adrenal tumors or hyperplasia.
Treatment: The treatment of Conn’s Syndrome aims to normalize blood pressure and electrolyte balance:
- Medications: Aldosterone receptor antagonists, such as spironolactone or eplerenone, can help block the effects of excess aldosterone, leading to improved blood pressure and potassium levels.
- Surgery: If the condition is caused by an adenoma, surgical removal of the tumor (adrenalectomy) is often considered. This can lead to a complete resolution of the symptoms.
Conn’s Syndrome, if left untreated, can contribute to long-term complications such as cardiovascular issues, kidney damage, and electrolyte disturbances. Timely diagnosis and appropriate management are essential to prevent these complications and improve overall health.
Pheochromocytoma
Pheochromocytoma is a rare and typically non-cancerous tumor that develops in the adrenal medulla, the inner part of one or both adrenal glands. These tumors are responsible for excessive production of catecholamines, which include adrenaline (epinephrine) and norepinephrine.
As a result, pheochromocytoma can have profound effects on the body’s sympathetic nervous system, leading to a range of symptoms and potentially life-threatening complications.
Key Points:
- Hormone Production: Pheochromocytomas produce excessive amounts of catecholamines, which are responsible for the “fight or flight” response in the body. This leads to a surge in blood pressure and various other symptoms.
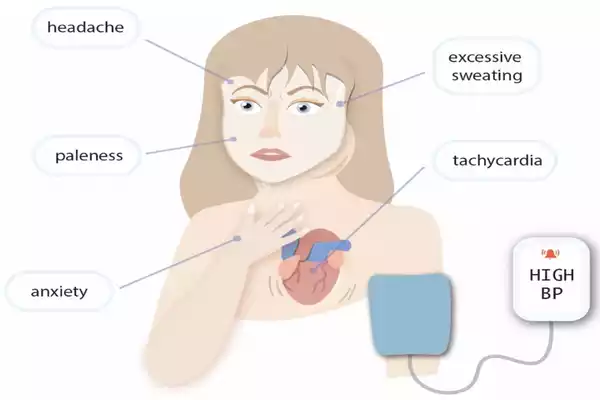
- Symptoms: The most common symptoms of pheochromocytoma include:
- Paroxysmal Hypertension: Sudden, severe spikes in blood pressure that can lead to headaches, sweating, and palpitations.
- Palpitations: Rapid and strong heartbeat.
- Sweating: Profuse sweating, often described as diaphoresis.
- Anxiety and Panic Attacks: Due to the surge in adrenaline.
- Headaches: Severe, pounding headaches.
- Tremors: Shaking or trembling, particularly in the hands.
- Episodic Nature: Pheochromocytoma symptoms often occur in episodes, triggered by stress, physical activity, or other factors that stimulate the release of catecholamines.
- Diagnosis: Diagnosis involves a combination of blood and urine tests to measure elevated catecholamine levels. Imaging studies, such as CT scans, MRIs, or MIBG scans, are used to locate the tumor.
- Treatment: The primary treatment for pheochromocytoma is surgical removal of the tumor (adrenalectomy). Before surgery, patients are typically given medications, such as alpha and beta-blockers, to control blood pressure and symptoms. This is crucial because manipulating the tumor or even undergoing surgery without proper preparation can lead to dangerous surges in blood pressure.
- Malignancy Risk: Most pheochromocytomas are benign (non-cancerous), but a small percentage can be malignant (cancerous). Malignant cases tend to be associated with a worse prognosis and may require additional treatments like chemotherapy or radiation therapy.
- Hereditary Syndromes: Some cases of pheochromocytoma are associated with hereditary genetic syndromes, such as multiple endocrine neoplasia type 2 (MEN2), von Hippel-Lindau (VHL) syndrome, or neurofibromatosis type 1 (NF1). In these cases, individuals may develop multiple tumors, and regular screening is crucial.
- Prognosis: If diagnosed and treated promptly, the prognosis for most individuals with pheochromocytoma is excellent. Surgical removal of the tumor typically leads to the resolution of symptoms.
- Follow-up: After surgery, patients often require ongoing monitoring to ensure that the tumor does not recur and that blood pressure remains controlled.
pheochromocytoma is a rare adrenal gland tumor that leads to the overproduction of adrenaline and norepinephrine, causing severe hypertension and a range of symptoms. Timely diagnosis, appropriate medical management before surgery, and surgical removal of the tumor are key to successful treatment and a good prognosis.
Conn’s Syndrome and Pheochromocytoma in the comparison chart
Here’s a brief comparison chart highlighting the key differences between Conn’s Syndrome and Pheochromocytoma:
| Characteristic | Conn’s Syndrome | Pheochromocytoma |
|---|---|---|
| Hormone Overproduced | Aldosterone | Catecholamines (Adrenaline, Norepinephrine) |
| Primary Symptom | Hypertension | Paroxysmal (Sudden, Severe) Hypertension |
| Electrolyte Imbalances | Hypokalemia (Low Potassium) | Generally normal electrolytes, unless a crisis |
| Common Symptoms | Muscle Weakness, Fatigue, Polyuria | Palpitations, Sweating, Tremors, Headaches |
| Triggering Factors | Not typically triggered by stress | Episodes are often triggered by stress, exercise, or other factors |
| Tumor Location | Aldosterone-producing adenoma or hyperplasia of adrenal glands | Adrenal medulla (chromaffin cells) |
| Malignancy Risk | Rarely malignant (usually benign) | Generally benign, but rare malignant cases exist |
| Diagnostic Tests | Elevated aldosterone levels, aldosterone-to-renin ratio | Elevated catecholamine levels in blood and urine |
| Imaging Studies | CT scan or MRI to locate the adrenal tumor | CT scan or MRI to locate the adrenal tumor |
| Treatment | Medications (aldosterone antagonists), surgery (adrenalectomy) | Medications (alpha and beta-blockers), surgery (tumor removal) |
| Prognosis | Good with appropriate treatment | Good with prompt diagnosis and surgical intervention |
| Hereditary Syndromes | Rarely associated with hereditary genetic syndromes | Occasionally associated with genetic syndromes (e.g., MEN2) |
Both Conn’s Syndrome and Pheochromocytoma are adrenal gland disorders with distinct hormonal imbalances and clinical presentations. Accurate diagnosis and appropriate management are essential to prevent complications and ensure the best possible outcomes for individuals with these conditions.
Importance of distinguishing between Conn’s Syndrome and Pheochromocytoma
Distinguishing between Conn’s Syndrome and Pheochromocytoma is crucial due to the following reasons:
- Treatment: Each condition requires specific treatments. Conn’s Syndrome may involve medications or surgery, while Pheochromocytoma requires preoperative management to control blood pressure before tumor removal.
- Complications: Failure to distinguish between the two can lead to inappropriate treatments, potentially worsening hypertension or causing dangerous hypertensive crises in Pheochromocytoma.
- Prognosis: Accurate diagnosis ensures appropriate management, improving the chances of successful treatment and minimizing long-term health risks for patients.
- Hereditary Factors: Recognizing these conditions aids in identifying underlying genetic syndromes that may impact the patient and their family’s health.
- Quality of Life: Properly managed, individuals can experience a better quality of life with controlled symptoms and minimized health risks.
Distinguishing between Conn’s Syndrome and Pheochromocytoma is essential for providing tailored care, preventing complications, and improving the overall well-being of patients.
Differential Diagnosis Challenges
- Similar Symptoms: Conn’s Syndrome and Pheochromocytoma share some common symptoms, such as hypertension and fatigue, which can make it challenging to distinguish between them based solely on clinical presentation.
- Overlap with Other Conditions: The symptoms of both conditions can mimic those of other medical conditions, including essential hypertension and anxiety disorders, leading to misdiagnosis or delayed diagnosis.
- Atypical Presentations: Some individuals with these disorders may not exhibit classic symptoms, making diagnosis even more challenging. For example, not all Pheochromocytoma patients experience paroxysmal hypertension.
- Coexistence: In rare cases, individuals may have both Conn’s Syndrome and Pheochromocytoma simultaneously, further complicating the diagnostic process.
- Hereditary Syndromes: Both conditions can be associated with genetic syndromes, necessitating a thorough evaluation of family history and genetic testing to uncover underlying causes.
Given these challenges, healthcare professionals must rely on a combination of clinical evaluation, hormone testing, and imaging studies to accurately diagnose and differentiate between Conn’s Syndrome and Pheochromocytoma.
Conclusion
Conn’s Syndrome and Pheochromocytoma are adrenal gland disorders with distinct characteristics. While their symptoms may overlap, accurate diagnosis is essential for appropriate treatment. Healthcare professionals must navigate challenges in differential diagnosis to ensure timely interventions and improved patient outcomes.